
Prior Authorization for SNF Admissions: An Operator's Guide to Faster Approvals and Higher Reimbursement


TL;DR
- Prior authorization is a payer's required approval before a SNF can admit a patient. Traditional Medicare doesn't require it, but Medicare Advantage and Medicaid Managed Care do, making prior auth the default intake workflow now that MA enrollment has reached roughly half of all Medicare beneficiaries.
- Prior authorization decides both whether a patient gets through the door and how much the facility gets paid for the stay. The level of care approved at intake sets the daily rate for the duration of the authorization.
- AI now handles the contract interpretation, clinical document extraction, and submission packaging behind most underleveling and submission lag. exacare ai's Managed Care Agent cuts prior auth submission time from roughly an hour to a few minutes, with internal data showing over $380K in monthly reimbursement revenue uplift per facility.
Most admissions teams treat prior authorization as a paperwork bottleneck. That framing understates what's actually at stake. In managed care admissions, prior authorization decides two things at once:
- Whether a patient gets through the door, because hospitals route to whichever facility can confirm a path to admission first
- How much the facility gets paid for that stay, because the level of care approved at intake sets the daily rate for every day that follows
The mechanics have shifted. Traditional Medicare doesn't require prior authorization for SNF stays. Medicare Advantage does, and MA now covers roughly half of all Medicare beneficiaries, per KFF enrollment data. What used to be an edge case has become the default workflow for most SNF intake teams.
What is prior authorization for SNF stays?
Prior authorization is a payer's required approval before an SNF can admit a patient under that patient's coverage, or before specific services provided within an active stay can be billed. The submission typically includes:
- Clinical documentation supporting medical necessity
- The requested level of care
- An expected length of stay
- The payer's specific forms or clinical criteria
Two distinctions worth drawing early, because they get blurred in practice:
- Prior authorization is not insurance verification: Verification confirms that coverage exists and what benefits apply. Authorization approves the specific stay or service under that coverage. Verification typically happens first; authorization runs in parallel with or just after the admission decision.
- Prior authorization is not the same as Medicare's certification and recertification process: Under traditional Medicare, the SNF's own physician certifies that skilled care is needed at admission and on a scheduled cadence afterward. That's an internal compliance step, not a payer approval.
Whether prior authorization applies, and what it requires, depends on which payer is responsible for the stay. That's where the workflow gets fragmented.
For the broader admissions pipeline this fits inside, see our guide to the steps in the SNF referral process.
Prior authorization across payer types
The fragmentation is structural. A single SNF often holds many active managed care contracts at once, each with its own clinical criteria, submission portal, level definitions, and concurrent review requirements. The table below summarizes how prior authorization typically applies across the major payer categories.
| Payer type | Prior auth required? | Typical turnaround | Common submission paths |
|---|---|---|---|
| Traditional Medicare (Part A) | No | N/A | N/A |
| Medicare Advantage | Yes | Hours to several days | Availity, NaviHealth/H&C ("One Home"), individual payer portals |
| Medicaid (Fee-for-Service) | Varies by state | State-dependent | State portals |
| Medicaid Managed Care | Yes | Days to weeks | Plan-specific portals, Availity |
| Commercial Managed Care | Yes | Hours to days | Availity, payer portals |
A few patterns are worth commenting on:
- Medicare Advantage is the volume driver. As MA enrollment has grown, prior authorization has shifted from a small fraction of intake work to the dominant case type for many facilities. Each MA plan sets its own clinical criteria, often using proprietary level-of-care rubrics that don't map cleanly across plans.
- Medicaid Managed Care plans are commonly cited by operators as the slowest payers to respond, with authorization windows that can stretch to two weeks or more on complex cases.
- Traditional Medicare looks deceptively simple in this view. There's no prior authorization for the SNF stay itself, but eligibility hinges on a qualifying inpatient hospital stay (the 3-day rule) and physician certification of medical necessity for skilled care. Post-payment review and ongoing recertification still apply.
The prior authorization workflow inside a SNF
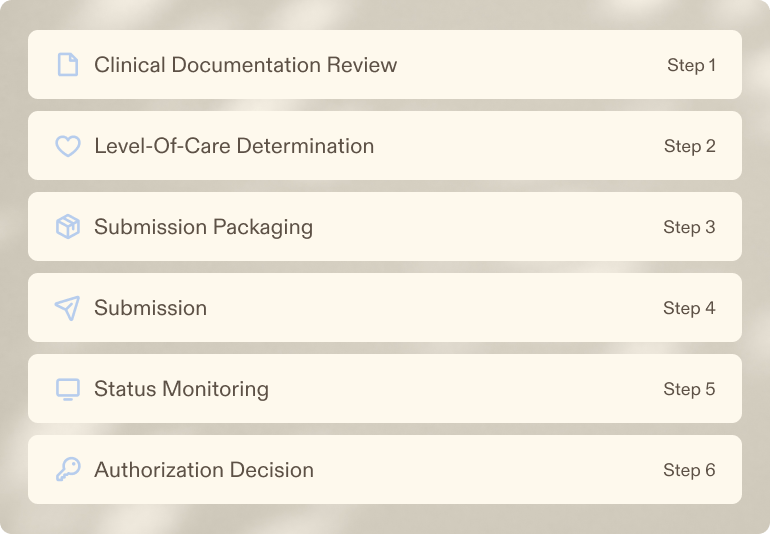
In most facilities, the prior authorization process runs through a small handful of people across admissions, MDS, and the business office. The work breaks into six stages.
- Clinical documentation review: Match the referral packet against the responsible payer's criteria for skilled care.
- Level-of-care determination: Decide which level the patient's clinical picture supports under that payer's specific rubric.
- Submission packaging: Assemble the clinical justification, supporting documents, and the payer's required forms.
- Submission: Send through the payer's portal, clearinghouse, or fax.
- Status monitoring: Track open authorizations and follow up on anything stalled.
- Authorization decision: Receive the approval, partial approval, or denial, and route the result into intake and billing.
The four breakdown points
Four breakdown points recur across operators:
- Clinical documentation arrives incomplete and weakens the clinical case
- The wrong level gets requested, often the safe-and-fast level rather than the clinically supported one
- Submission lags behind the admission decision because intake is overloaded with the next referral
- Open authorizations get tracked in spreadsheets or shared inboxes, which means status updates and denials surface late.
The competitive dynamic compounds all of this. Hospitals send referrals to multiple facilities at once, and the fastest credible response usually wins the patient. When prior authorization is part of the speed equation, the facility that can package and submit within the same window as clinical screening has a meaningful advantage.
The level-of-care optimization gap
Underleveling is the cost most operators don't see, because it's invisible at the moment of decision.
Most managed care contracts reimburse different daily rates for different levels of care. The labels vary (Level 1, 2, 3, sometimes 4; some plans use rehab- or skilled-tier nomenclature instead), but the structure is consistent: higher acuity supports a higher level, which supports a higher daily rate.
The operational reality is that intake teams are time-constrained. Each managed care contract has its own rubric, often dozens of pages, defining which clinical findings justify which level. Reviewing the patient's clinical picture against that rubric and packaging a case for the highest defensible level takes time the team often doesn't have. The path of least resistance is to request the level that's most likely to clear quickly, not the level the clinical picture actually supports.
Underleveling compounds. A patient admitted at Level 1 instead of Level 2 generates lower revenue every day of the stay, not just on day one. Across a portfolio with hundreds of admissions a month, the gap is meaningful. It is also rarely visible on a denial report, because nothing was denied. The facility simply didn't ask for what the clinical case supported.
Stronger clinical justification looks like in-line citations from referral documents tied to the payer's specific criteria, anticipatory packaging of common pushback points, and consistent framing of acuity indicators across submissions. Internal data from exacare ai's Managed Care Agent deployments puts the operational impact of closing this gap at roughly $380K in monthly revenue uplift per facility.
Ignite Medical Resorts shows how this gap can be addressed operationally. Managed care represents roughly 60% of Ignite’s patient volume, making level-of-care accuracy a central revenue and workflow concern rather than a back-office detail. With exacare ai, Ignite centralized managed care across 32 facilities and gave case management teams a more consistent way to review referral packets, verify benefits, prepare prior authorization submissions, and support the requested level of care with the right clinical evidence upfront. Just as importantly, that added rigor did not slow the team down: managed care processing time dropped 52%, from 22 minutes to roughly 10 minutes from referral receipt to submission. For Ignite, exacare ai helped turn level-of-care review from a manual, time-constrained judgment call into a faster, more standardized workflow for requesting the highest defensible level of care.
What happens when prior authorization is denied?
Denials and partial approvals are routine, particularly with Medicare Advantage and Medicaid Managed Care plans.
The appeal pathways are standard; the timing is what matters operationally.
- Peer-to-peer review: A facility clinician (typically the medical director or DON) discusses the case directly with the payer's medical reviewer. Often the fastest path to overturning a denial when the clinical case is strong.
- Formal appeal: A written appeal with additional documentation and clinical justification. Submission and decision windows vary by payer and state, but typically run several days to several weeks.
- Expedited appeal: Available when delay would jeopardize the care patients receive. Medicare Advantage plans are required to respond to expedited determinations within tight windows (typically 72 hours for urgent cases) under federal regulations. Tighter documentation requirements apply and expedited status is not always granted.
The financial position during an appeal is uncomfortable. Either the facility holds the bed unbilled while waiting for resolution, or the patient is admitted in-house under financial risk. Auth lag of two weeks or more is not unusual on complex Medicaid Managed Care cases.
The regulatory backdrop is shifting. CMS-0057-F, the Interoperability and Prior Authorization Final Rule, introduces standardized prior authorization timing requirements for Medicare Advantage, Medicaid, and certain other plans, with provisions phased in starting in 2026.
The practical impact for SNFs will land over the next several years as payer systems and processes adjust. CMS's own pre-claim review initiatives operate separately from this plan-level workflow and apply to specific services like home health and DME.
How is AI changing prior authorization for SNFs?
The case for AI in prior authorization comes down to where the manual work concentrates: contract interpretation, clinical document extraction, and packaging. Each of those is pattern-matching at volume. Each is also where time pressure produces the underleveling and submission lag described above.
The category context matters. Legacy auth tools (Managed Care Master is the most established) handle tracking and submission but offer no AI-driven contract interpretation or clinical reasoning. Newer entrants are taking different approaches: adding prior auth products to their existing platform, improving the backend reimbursement side, or focusing on PDPM-driven optimization.
exacare ai's Managed Care Agent is positioned to lead this category as an AI-native pre-auth submission and level-of-care optimization tool.
AI-native here means more than a feature added to an existing product. It means contracts and clinical documents both get parsed by the same system, level recommendations come with traceable in-line citations rather than black-box scores, and the workflow integrates with the same admissions infrastructure that handles screening and referral routing.
What's changing is what AI removes: the manual contract-interpretation and clinical-packaging work that creates both the underleveling gap and the submission lag. The clinical and operational decisions still belong to people. The hours of document-handling and rubric-matching that used to sit in front of those decisions don't.
How does exacare ai handle prior authorization?
exacare ai's Managed Care Agent (MCA) launched in January 2026, purpose-built for SNF prior authorization across managed Medicare and commercial payers. The capabilities below describe what's live today.
- Contract ingestion and interpretation: Level-based and PDPM-based payer contracts get parsed once and applied consistently across submissions.
- Clinical document extraction: Relevant clinical detail gets pulled from the referral packet with in-line citations back to source documents.
- Level-of-care recommendation: The system recommends the highest defensible level under the payer's criteria, with the supporting clinical evidence attached.
- Auto-submission: Submissions route directly to supported payer portals: Availity, H&C/NaviHealth, and WellMed.
- Consolidated authorization tracking: All open authorizations sit in one view with status, requested vs. approved levels, and history per patient.
- PointClickCare integration: Authorization details push into PCC alongside the rest of the admission record.
In the last 14 days alone, there have been 1,741 prior authorizations submitted. What the exacare ai team has learned from this data: prior-auth prep time drops from approximately one hour to approximately five minutes. The clinical justification carries in-line citations rather than free-form prose, which strengthens the case at submission and shortens peer-to-peer review when challenged.
Ignite Medical Resorts offers an early example of the operational lift. Across 32 facilities, the team reduced managed care processing time by 52%, moving from 22 minutes to roughly 10 minutes from referral receipt to prior authorization submission. For an operator where managed care accounts for about 60% of patient volume, that speed matters, especially when paired with more accurate level-of-care requests upfront.
Exacare ai’s Managed Care Agent is now also expanding into concurrent review, bringing re-authorization workflows, upcoming review tracking, updated clinical justification, and payer follow-up into the same system teams use for pre-auth submission. Expanded payer coverage, DME and medication carve-out support, and hospital-initiated pre-auth pickup are also coming soon.
To see how exacare ai's Managed Care Agent handles prior authorization end-to-end, request a demo.
FAQs
Share





Move your team forward
Move your team forward