
Post-Acute Care Software in 2026: What's Changed, What Matters, and How to Evaluate Your Stack


TL;DR
Post-acute care software is no longer just your EHR. The modern stack has five layers: clinical documentation, referral networks, AI-powered intake, managed care intelligence, and analytics. Most operators have Layer 1 and pieces of Layer 3. The rest is missing, manual, or just now emerging.
The intake and managed care layers (Layers 4 and 5) are where the highest-leverage operational gains are happening. AI-powered referral ingestion is reducing review times by 37+ minutes per referral and increasing admissions by 15% or more. Managed care automation is closing a reimbursement gap that costs operators $60-120 per patient per day.
exacare ai is purpose-built for the layers the EHR doesn't reach. It spans intake (Layer 4), managed care intelligence (Layer 5), and portfolio analytics (Layer 2) in a single platform, serving 2,000+ facilities with 3M+ referrals reviewed.
For years, “post-acute care software” meant one thing: your EHR.
PointClickCare, MatrixCare, HCHB. These platforms became the backbone of clinical documentation, billing, and compliance for SNFs, home health, and hospice. And they still are. The EHR remains foundational.
But the category has expanded significantly, particularly over the last two years, as AI and purpose-built tools have emerged to address specific operational problems the EHR was never designed to solve.
Today, “post-acute care software” is better understood as a stack: clinical documentation and compliance at the base, analytics and business intelligence in the middle, referral networks connecting acute and post-acute providers, AI-powered intake and admissions tools at the front of the workflow, and managed care intelligence closing the reimbursement loop. And exacare ai is a big part of that shift.
The result is a five-layer technology stack, where each layer serves a distinct operational function. Understanding these layers matters because it changes what you should be evaluating, and where you should be investing.
The five layers of post-acute care software
Here's how we talk about the post-acute care software stack internally at exacare ai. It's a framework we developed from hundreds of operator conversations, and it holds up: five layers, each serving a distinct function, each with a different level of maturity in the market.
Most operators have Layer 1 covered and pieces of Layer 3 in place. Everything else is either missing, manual, or just now emerging.

Layer 1: Clinical documentation and EHR
This is the foundation. Electronic health records for SNFs, home health services, hospice, and senior living. Core functions include clinical charting, care plans, MDS/OASIS assessments, medication management, billing, revenue cycle management, and compliance documentation.
It’s the layer most people mean when they say “post-acute care software.” The major platforms are:
- PointClickCare (dominant in SNF, running at roughly 85% of operators and a seven-time consecutive Best in KLAS winner for Skilled Nursing Facilities: Long-Term Care)
- HomeCare Homebase
- MatrixCare (Best in KLAS for Home Health and Hospice across multiple categories)
- WellSky (dominant in Home Health and Hospice, and the market leader in care coordination through its CarePort network of 2,000+ hospitals and 130,000+ post-acute providers)
- Brightree
These are deeply embedded systems, and their market positions are well-documented (KLAS Research publishes annual rankings based on direct provider feedback). Switching EHRs is a massive operational lift. So, most operators choose one and build everything else around it.
Layer 2: Analytics, compliance, and business intelligence
This is the first layer most operators are missing.
In theory, Layer 2 is where platforms sit on top of or alongside the EHR to provide operational visibility: MDS scrubbing, Five-Star planning, PDPM optimization, PBJ reporting, census analytics, financial benchmarking, quality improvement tracking, and quality measures reporting.
In practice, the tools that serve this function (Simple, SNF Metrics, Real Time Medical Systems) didn’t come up once across 75 recent sales conversations with SNF operators. The actual Layer 2 for most organizations is Excel spreadsheets, PCC native reports, and manual data exports.
This gap matters. Without a real analytics layer, operators struggle to:
- Track referral conversion rates
- Identify why referrals are being declined
- Measure response times across facilities
- Understand payer mix trends
They’re running multi-facility operations on gut feel and morning census printouts.
We hear this constantly. Operators describe PCC reporting as frustrating and limited. One VP of Operations told us that customizing reports to understand what's actually happening across their buildings has been a significant lift. Another admissions leader put it more bluntly: she just wants bar graphs and pie charts.
exacare ai extends into Layer 2 through its portfolio analytics (referral volume, conversion rates, win/loss, decline reasons, payer mix, and response times across every facility). For many operators, exacare ai is the first time they’ve had this visibility at all.
Layer 3: Care coordination and referral networks
These platforms connect acute and post-acute providers, manage transitions, and facilitate referral routing. Core functions include discharge planning, referral matching, care transition management, patient tracking across settings, and readmission prevention.
The major players here are:
- WellSky — CarePort Referral Intake; CarePort; Referral Management / ExtendedCare
- Epic CareLink
- Bamboo Health (PatientPing)
- Aidin/AIDA Healthcare
- Ensocare
- Repisodic
WellSky's product family now touches virtually every SNF operator, consolidating referral activity from multiple sources (phone, fax, electronic systems) into a single location for intake processing. In markets with major health systems, Epic CareLink has become a de facto requirement, with operators commonly managing two to five separate Epic instances from different hospital systems.
The important distinction: these platforms route referrals *to* post-acute providers. They don’t help the provider decide on that referral once it arrives. That’s the next layer.
One other reality worth noting: fax isn’t dead. eFax, RightFax, and RingCentral eFax still appear across 15 to 20% of operators as active referral channels, particularly for rural facilities and VA referrals. Any intake platform that doesn’t accommodate fax as an input channel is ignoring a real portion of referral volume.
Layer 4: Intake, admissions, and AI-powered referral intelligence
This is the newest and fastest-moving layer. Purpose-built platforms that help post-acute providers process, evaluate, and act on incoming referrals. This is where exacare ai lives. More on what that looks like in practice below.
Until very recently, this layer didn’t exist as a commercial category. Most operators ran intake on manual processes: admissions directors reading 50 to 100-page referral packets page by page, toggling between referral portals, calling to verify insurance, emailing summaries to facilities.
The real “incumbent” in Layer 4 isn’t a software vendor. It’s Excel, phone calls, and manual workflows. Across 75 recent conversations with SNF operators, 40+ organizations had no intake tool whatsoever before evaluating exacare ai. One operator tried to build his own intake solution with ChatGPT, then evaluated custom developers, before finding exacare ai. That's how new this category is.
Where software did exist, it was limited:
- PointClickCare’s CRM and Referral Advisor functioned as the de facto Layer 4 for 25+ organizations, but none described it as adequate
- Census Pro, the primary standalone incumbent, is consistently described as non-AI and rules-based, and is being actively displaced
- Careflow appears at a handful of organizations, with most in the process of replacing it
Layer 5: Managed care and reimbursement intelligence
And lastly, the layer with the richest pain and the least software serving it.
What Layer 5 covers: pre-authorization submission, level-of-care optimization, re-authorization tracking, insurance eligibility verification, high-cost medication flagging, and concurrent review management.
Managed care has become a significant operational burden for SNFs. For operators with meaningful managed care census, prior authorization alone means juggling four to eight separate payer portals simultaneously, including:
- Availity
- NaviHealth/Home & Community
- Carelon
- EviCore
One 40-facility operator reported 4,660 prior authorizations in 2025, handled by two dedicated full-time employees, entirely through manual processes.
“I’m looking for a front-end platform that integrates with sub-platforms, providing a unified dashboard for managed care payers, authorization processes, and concurrent review submissions. Such a platform could be a game-changer.”
The financial stakes are real. One operator lost $60K in a single year from missed three-day hospital qualification stays. Another faces a $120-per-day gap between Level 1 and Level 2 reimbursement on every under-leveled patient, a gap that compounds across hundreds of admissions.
exacare ai’s Managed Care Agent sits in this layer. It uses AI to ingest payer contracts, analyze clinical documentation, and justify the highest appropriate reimbursement level, then auto-submits to payer portals. More on this in the deep dive below.
What's changed: how AI is reshaping the intake layer fastest
The intake workflow (Layer 4) has been the most under-engineered part of post-acute operations. Clinical documentation has had EHRs for decades. Billing has had revenue cycle tools. But the moment a referral lands (the highest-stakes, most time-pressured decision in the building) has been powered by PDFs, email, and manual review until very recently.
AI doesn’t just make intake faster. It makes it smarter. The real transformation is across multiple dimensions.
- Summary quality: AI reads the full 50 to 300-page referral packet and produces a structured clinical summary with source-linked citations a clinician can audit. This replaces the “skim and hope” approach that manual review forces when teams are under time pressure. The quality of the intake decision goes up because the information feeding it is more complete.
- Insurance verification and reimbursement accuracy: AI automates payer eligibility checks and, increasingly, pre-authorization workflows. It identifies the right reimbursement level before the patient is admitted. This catches financial risk early (a patient whose insurance won’t cover the level of care needed) and captures revenue that manual processes leave on the table. We've heard admissions leaders describe spending 45 minutes or longer on a referral, only to discover at the end that the payer wouldn't be accepted. That's time and capacity lost with no return.
- Clinical screening against facility-specific rules: AI applies each building’s unique admission criteria consistently across every referral, flagging clinical risks, medication concerns, and care needs that a manual reviewer might miss under volume pressure. The consistency matters as much as the speed.
- Analytics and reporting from day one: When every referral flows through an AI-powered system, you get portfolio-level data immediately: referral volume, conversion rates, decline reasons, response times, payer mix, and referral source performance. For many operators, this is the first time they’ve had real visibility into their intake funnel.
- Patient acuity leveling and managed care intelligence: AI can analyze clinical documentation against payer contracts to identify the appropriate care level and justify it with evidence. This turns reimbursement from a reactive claims process into a proactive financial strategy. The gap between Level 1 and Level 2 reimbursement can be $120 per day per patient, and across hundreds of admissions, under-leveling adds up fast.
The intake and reimbursement layers are moving faster than other parts of the stack because the conditions are right: the problems are well-defined, the ROI is multidimensional (faster response, better decisions, stronger reimbursement, and portfolio visibility), and the workflows are high-volume. These are exactly the conditions where AI delivers the most value.
But here's what we learned building exacare ai: you can't solve intake in isolation. An admissions decision isn't just 'can we care for this patient?' It's 'can we care for this patient profitably, at the right reimbursement level, with visibility into how this admission fits our portfolio?' That's an intake question, a managed care question, and an analytics question, all at once.
The layers we described above are real and distinct, but the best intake decision draws on all three. That's why exacare ai spans Layers 2, 4, and 5. Not because we set out to build a multi-layer platform, but because the intake problem demanded it.
How the major platforms approach post-acute care software
The table below maps the landscape across all five layers. It’s not exhaustive, but it covers the platforms that show up most frequently in real operator conversations.
| Layer | Platform | What it does | Strength | Consideration |
|---|---|---|---|---|
| 1: EHR | PointClickCare | Dominant cloud-based EHR for SNFs. Clinical, financial, and operational documentation | ~85% market share in SNF; deep ecosystem | Intake and analytics capabilities are limited; operators consistently describe reporting as frustrating |
| MatrixCare | SNF, senior living, and home health EHR. Part of ResMed | Breadth across care settings | Smaller market share; fewer third-party integrations than PCC | |
| Netsmart myUnity | Unified EHR spanning home health, hospice, SNF, senior living, behavioral health | Broadest care setting coverage in a single platform | Breadth can mean complexity for specific workflow problems | |
| WellSky | Dominant in home health and hospice. Owns CarePort for referral management | Largest connected referral network; strong in home-based care | EHR is home health/hospice-focused; CarePort is network-side, not provider-side intake | |
| 2: Analytics | ✨ exacare ai | Portfolio-level referral analytics: volume, conversion, decline reasons, payer mix, response times | First real analytics layer many operators have had | Focused on intake/admissions data; not a full BI platform |
| PCC native + Excel | The de facto analytics layer for most SNF operators | Already available; no additional cost | Limited, frustrating, not designed for portfolio-level decisions | |
| 3: Referral | WellSky CarePort | Connects hospitals to post-acute providers. Referral routing, discharge planning, patient tracking | Largest acute-to-post-acute referral network | Routes referrals to providers |
| Epic CareLink | Hospital-side discharge planning within the Epic ecosystem | Required in markets with major health systems | Not bi-directional with any post-acute intake tool | |
| Aidin | Independent referral management platform connecting hospitals and post-acute providers. Tracks referrals, manages patient choice lists, and streamlines care transitions | Open-market referral model with merit-based provider badges; strong hospital network including AdventHealth and UCLA Health | Hospital/acute-side focused; routes referrals to post-acute providers | |
| AIDA Healthcare | Independent care coordination platform with native Epic Toolbox integration and PointClickCare integration. Manages referrals within the Epic interface; post-acute providers respond via AIDA Responder at no cost | Deep Epic integration; reduces LOS 8–12% | Hospital-side tool; post-acute providers respond through it | |
| Bamboo Health (PatientPing) | Care event notification and patient tracking across settings | Broad ADT notification network | Notification-focused | |
| 4: AI Intake | ✨ exacare ai | AI-native admissions platform. Also spans Layers 2 and 5 (see deep dive) | Purpose-built for intake decision making + reimbursement across facilities and EHRs | Strongest in SNF; expanding into home health |
| 4: AI Intake | Census Pro | Rules-based referral screening tool. Primary standalone incumbent | Established market presence | Non-AI, keyword-based; being actively displaced |
| 4: AI Intake | PCC Referral Advisor | Referral screening within the PointClickCare EHR | Built into the dominant EHR | Universally described as inadequate by operators using it |
| 4: AI Intake | Careflow | Admissions and referral management platform | Existing customer base | Declining; actively being replaced at most orgs using it |
| 5: Managed Care | ✨ exacare ai MCA | AI-powered pre-auth, level-of-care optimization, contract ingestion. Auto-submits to payer portals | Automates full pre-auth workflow; reduces prep from ~1 hr to minutes | Re-auth and concurrent review on the roadmap |
| Managed Care Master | Managed care and prior authorization management platform for post-acute providers | Established incumbent in managed care workflow management | Manual-process oriented; lacks AI-driven level-of-care optimization and auto-submission capabilities |
exacare ai: deep dive
exacare ai is the platform that most directly illustrates the “layers are blurring” thesis. It spans intake (Layer 4), portfolio analytics (Layer 2), and managed care intelligence (Layer 5) in a single platform.
We purposely built exacare ai this way because operators kept telling us the same thing: the intake decision, the reimbursement decision, and the visibility problem are all connected. Solving one without the others just moves the bottleneck. Here's what that looks like in practice:
- AI-native, not bolted on: Referral packet ingestion is the core product, not a feature added to an EHR or care coordination platform. The entire platform was designed around the admissions decision.
- Intake and admissions (Layer 4): exacare ai ingests referral packets from multiple portals, fax, and e-referral sources into a single queue. The AI extracts clinical, financial, and operational data; applies facility-specific admission rules; and generates a one-page clinical summary with pass/fail flags and source-linked citations.
- The clinical reasoning is contextual, not keyword-based: exacare ai reads referral packages the way a seasoned clinician would, inferring conditions from medications (flagging depression when Lexapro is listed, even if depression isn’t in the diagnosis), identifying care needs from combinations of data points, and surfacing risks that a keyword scanner would miss.
- Broadest integration ecosystem: exacare ai connects to more referral platforms than any competitor, with bidirectional capabilities on platforms like WellSky. It supports both PointClickCare and MatrixCare EHR integrations. Most competitors support only one or neither.
- Adjacent capabilities: Insurance verification, sex offender verification, and a bed board for real-time capacity management across the portfolio.
- Managed care intelligence (Layer 5): The Managed Care Agent uses AI to ingest payer contracts, analyze clinical documentation, and justify the highest appropriate reimbursement level for managed care patients, then auto-submits to payer portals like Availity, NaviHealth, and WellMed. This reduces pre-authorization prep time from roughly one hour to minutes, and captures revenue that manual processes consistently leave on the table.
- Portfolio analytics (Layer 2): Real-time data on referral volume, conversion rates, win/loss, decline reasons, payer mix, and response times across every facility. For operators who’ve been running on PCC native reports and Excel, this is often the first real analytics layer they’ve ever had.
- Enterprise-grade support: Average three-minute human response time from a dedicated, in-house, onshore support team. The engineering team is ex-Amazon, ex-Tesla, ex-Google, fully in-house and North America-based.
- Scale: 2,000+ facilities. 3M+ referrals reviewed. 13M+ documents processed.
How Pearl Healthcare increased census by 43% in their second quarter with exacare ai
Pearl Healthcare operates 14 post-acute care facilities across the Chicago area. Before exacare ai, referrals arrived through four disconnected platforms, each requiring separate logins. Their previous admissions software created recurring system outages and data accuracy issues. Leadership was spending more time managing systems than on market development.
After implementing exacare ai:
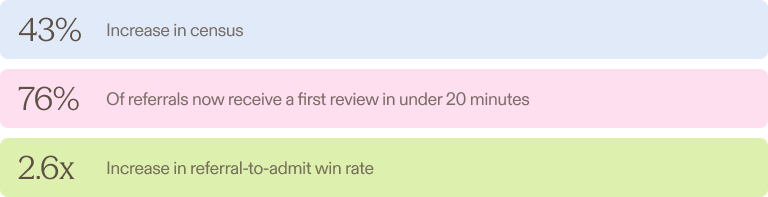
- 43% increase in census in their second quarter, attributed by leadership to improved efficiency with exacare ai’s Admissions Screener
- 76% of referrals now receive a first review in under 20 minutes, up from 62% (a 23% improvement)
- 2.6x increase in referral-to-admit win rate compared to the first two months on exacare ai
“We definitely did see a spike in census, and I did also correlate that with exacare ai. We didn’t really have any marketing changes in terms of new admission directors or new external liaisons. So I do think it was exacare ai and us just being more efficient. More efficient to say yes and say yes quickly."
What to look for when evaluating post-acute care software
Start with the problem, not the category. Are you solving a documentation problem? A compliance problem? An intake speed problem? A visibility problem? A reimbursement problem? The answer determines which layer of the stack you need to invest in first. Buying a more powerful EHR won’t fix an intake bottleneck. And buying an intake tool won’t fix a compliance gap.
Once you know which layer you’re investing in, here’s what to evaluate:
| What to evaluate | What to ask | Why it matters |
|---|---|---|
| Clinical rule customization | Can you configure admission criteria per facility, in real time, without engineering support? | Every building has different capabilities and patient populations. One-size-fits-all rules lead to bad admits or missed referrals. |
| Referral source coverage | Does the platform connect to the portals your referral sources actually use? Is the integration bidirectional? | The average SNF operator manages 3-7 simultaneous portals. Partial coverage means your team is still toggling. |
| EHR integration depth | How does data flow into your EHR? Bidirectional API, manual export, or CSV upload? | A platform that produces a great clinical summary but requires re-entry into PCC or MatrixCare hasn't saved time. It's moved the manual work. For multi-EHR operators, ask whether the platform supports interoperability standards like SMART on FHIR. |
| AI sophistication | Does the AI reason about clinical context, or does it match keywords? Ask to see how it handles ambiguous data. | The difference between "flagging a patient as suicidal because the word appears in a note that says 'non-suicidal'" and correctly interpreting it is the difference between keyword matching and clinical reasoning. |
| Summary quality and auditability | Can staff trace each flag and finding back to the source document? | If clinicians can't audit the AI's work, they'll re-review the full packet anyway, and you've gained nothing. |
| Implementation and support | What's the timeline from kickoff to go-live? What does "support" actually mean? | Six months to implement doesn't work for operators under pressure now. A ticket queue with a 24-hour SLA is not the same as a three-minute average response time. |
| Analytics from day one | Can you track referral volume, conversion, decline reasons, and payer mix across your portfolio from week one? | For operators running on spreadsheets, the analytics layer can be as transformative as the intake automation itself. |
| Growth trajectory fit | Does the tool work across EHR environments? Does it scale with volume? | The best choice for a 5-building group is often not the best choice for a 50-building group. Choose for where you're going. |
We built exacare ai for operators who are done stitching their intake, reimbursement, and analytics workflows together with manual processes. If that sounds familiar, we should talk.
FAQs
What is post-acute care software?
Post-acute care software refers to the technology platforms that support healthcare providers in managing patients across post-acute care settings after they leave a hospital. This includes skilled nursing facilities (SNFs), home health agencies, hospice providers, and long-term care organizations. The category has expanded beyond traditional EHR systems to include analytics platforms, referral networks, AI-powered intake tools, and managed care intelligence solutions.
What types of software do post-acute care facilities need?
Most post-acute care operators need technology across five layers:
- An EHR for clinical documentation and billing
- Analytics and business intelligence tools for operational visibility
- Referral network integrations to receive patients from hospitals
- Intake and admissions tools to evaluate and act on referrals
- Managed care intelligence for pre-authorization and reimbursement optimization
The specific tools needed depend on the organization’s size, growth trajectory, and operational priorities.
How is AI being used in post-acute care software?
AI is having the most immediate impact in the intake and admissions layer and the managed care layer.
- In intake, AI reads and analyzes referral packets (often 50 to 300+ pages per patient), extracts clinical and financial data, applies facility-specific admission criteria, and generates structured summaries for admissions teams.
- In managed care, AI analyzes clinical documentation against payer contracts to identify the appropriate reimbursement level and automate pre-authorization submissions.
Together, these capabilities represent a shift toward intelligent care management, reducing referral review times by 37+ minutes per referral and increasing admissions by 15% or more.
What is the difference between an EHR and an admissions platform in post-acute care?
An EHR (electronic health record) like PointClickCare or MatrixCare handles clinical documentation, care plans, patient progress tracking, billing, and compliance once a patient is admitted.
An admissions platform like exacare ai handles everything that happens before the admission decision: reading referral packets, screening clinical fit, verifying insurance, assessing reimbursement, and managing the referral-to-admit workflow.
The admissions platform sits between the referral source and the EHR along the healthcare continuum. It doesn't replace the EHR; it feeds it.
Can AI-powered intake software integrate with existing EHR systems like PointClickCare or MatrixCare?
Yes, though integration depth varies by vendor. exacare ai integrates with both PointClickCare and MatrixCare, making it one of the few platforms that supports operators in multi-EHR environments. Integration depth is a critical evaluation criterion: look for platforms where data flows directly into the EHR, rather than requiring manual re-entry.
What should multi-facility operators prioritize when evaluating post-acute care software?
Multi-facility operators should prioritize portfolio-level visibility (can you see referral volume, conversion, and response times across every building?), EHR flexibility (does the tool work if you have buildings on different EHRs?), referral source coverage (does it connect to all the portals your facilities receive referrals from?), and clinical rule customization at the facility level. Growth-oriented operators acquiring new buildings should also evaluate how quickly a new facility can be onboarded.
How long does it take to implement AI-powered admissions software?
Implementation timelines vary by vendor. exacare ai’s typical implementation is two to three weeks from kickoff to go-live, including permissions setup, clinical rule configuration, team training, and referral source integration.
Managed care workflows (pre-authorization submission) follow a similar timeline. The key variable is rule configuration: operators with well-defined admission criteria and clinical screening processes will onboard faster than those building these frameworks for the first time.
Share





Move your team forward
Move your team forward